I was saying "I'm the greatest” long before I believed it.
-Muhammad Ali
The word "motivation" is derived from the Latin "movere" which means "to move". Motivation refers to psychological forces which move people, bring them to an action and keep them going. Motivation explains the degree of the effort that is spent while performing an activity, the level of performance in achievement tasks and satisfaction and well-being that is derived from an activity and/or its outcome.
The three components of motivation as listed by Arnold et al (1991) are :
(i) Direction - what a person is trying to do
(ii) Effort - how hard a person is trying
(iii) Persistence - how long a person keeps on trying
There are two different categories of motivation theories such as content theories, and process theories. Content theory is also known as need theory. Another type of motivation theory is process theory. Process theories of motivation provide an opportunity to understand thought processes that influence behavior. The major process theories of motivation include Adams' equity theory, Vroom's expectancy theory, goal-setting theory, and reinforcement theory.
Need Theory
Also known as content theory, need theory of motivation mainly focuses on the internal factors that energize and direct human behavior. Maslow's hierarchy of needs, Alderfer's ERG theory, Herzeberg's motivator-hygiene theory (Herzeberg's dual factors theory), and McClelland's learned needs or three-needs theory are some of the major content theories.
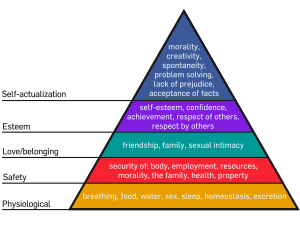 - Maslow's Hierarcy of Needs -
- Maslow's Hierarcy of Needs -
- Herzberg’s Two-Factor Theory -
Expectancy Theory
Expectancy theory is about the mental processes regarding choice, or choosing. It explains the processes that an individual undergoes to make choices. This theory was originally contained in the valency-instrumentality-expectancy (VIE) theory, proposed by Victor Vroom (1964).
Motivation is only likely when a clearly perceived and usable relationship exists between performance and outcome, and the outcome is seen as a means of satisfying needs. Vroom suggests that “for a person to be motivated, effort, performance and motivation must be linked”.
Motivation can be expressed as ; M = f(E*V), or as function of valence times expectancy.
This theory was then developed by Porter and Lawler (1968) into a model.

Lawler/Porter Diagram
Instrumental Theory
Another approach is known as the instrumental theory, pioneered by Goldthorpe and his colleagues' who concluded that for some people, work is only a means to gain financial reward.It stresses that for certain people, extrinsic reward such as high economis gains are valued more than intrinsic rewards like job satisfaction.
Goal Theory
Although setting goals was nothing new, it wasn't until the 1960s that an American called Dr Edwin Locke began to formally examine the relationship between motivation and the setting of goals. His main conclusions were :
John Stacey Adams, a workplace behavioural psychologist, put forward his Equity Theory on job motivation in 1963. When people feel fairly or advantageously treated they are more likely to be motivated; when they feel unfairly treated they are highly prone to feelings of disaffection and demotivation.
Social Learning Theory
The social learning theory of Bandura emphasizes the importance of observing and modelling the behaviours, attitudes and emotional reactions of others.

More :
1. Wikipedia
2. Evolution of a Motivation Theory
3. Motivation TheoryMotivation is only likely when a clearly perceived and usable relationship exists between performance and outcome, and the outcome is seen as a means of satisfying needs. Vroom suggests that “for a person to be motivated, effort, performance and motivation must be linked”.
Motivation can be expressed as ; M = f(E*V), or as function of valence times expectancy.
This theory was then developed by Porter and Lawler (1968) into a model.
Lawler/Porter Diagram
Instrumental Theory
Another approach is known as the instrumental theory, pioneered by Goldthorpe and his colleagues' who concluded that for some people, work is only a means to gain financial reward.It stresses that for certain people, extrinsic reward such as high economis gains are valued more than intrinsic rewards like job satisfaction.
Goal Theory
Although setting goals was nothing new, it wasn't until the 1960s that an American called Dr Edwin Locke began to formally examine the relationship between motivation and the setting of goals. His main conclusions were :
- specific goals are more motivating than vague goals.
- challenging goals are more motivating than easy goals.
- when people are given positive feedback, both during and after taking action on theor goals this spurs them to achieve even more.
John Stacey Adams, a workplace behavioural psychologist, put forward his Equity Theory on job motivation in 1963. When people feel fairly or advantageously treated they are more likely to be motivated; when they feel unfairly treated they are highly prone to feelings of disaffection and demotivation.
Social Learning Theory
The social learning theory of Bandura emphasizes the importance of observing and modelling the behaviours, attitudes and emotional reactions of others.
"Learning would be exceedingly laborious, not to mention hazardous, if people had to rely solely on the effects of their own actions to inform them what to do. Fortunately, most human behaviour is learned observationally through modelling : from observing others one forms an idea of how new behaviours are performed, and on later occasions this coded information serves as a guide for action."
-Albert Bandura (1977))
More :
1. Wikipedia
2. Evolution of a Motivation Theory
4. Motivation by Leslie Radford
5. Handbook of Human Resource Management Practice















{kind=link}
{kind=link}